The rate of caries progression in aged care facilities is often rapid!
Conventional dental treatment in aged care facilities is often unsuccessful due to many compounding factors. Treatment of the very frail and elderly, especially those suffering dementia, is a relatively new field and often not handled well. Root surfaces are particularly vulnerable sites for dental caries in the frail and elderly. By middle age many root surfaces are exposed as a result of gingival recession, and each exposed surface is a potential site for future caries. The transition between a sound root surface and a grossly carious one can be extremely rapid, sometimes measured in months.
Factors contributing to raise the caries rates in aged-care facilities.
- Often a catastrophic event such as a fall or a serious illness can impact and accelerate the deterioration of a person’s oral health.
- As a result of polypharmacy, some patients produce liquid in their mouth, but instead of having the buffering effect of saliva, because of the changes in saliva flow and production; the pH of the resting saliva of these patients is as low as 5.0-5.8 which is highly acidic, compared to moderately acidic saliva pH 6.0-6.6 and healthy saliva pH 6.8-7.8.
- The carbonate cycle that produces bicarbonate, responsible for the buffering action of saliva is disrupted in these patients, the saliva they produce is a liquid with no buffering ability, and is in fact a source of high acidity (pH 5.0-5.8), which usually can’t protect teeth surfaces effectively; this level of acidity in the mouth favours demineralization and/or increasing colonisation by acidophilic bacteria. That is why we see rampant caries in these elderly patients compromised by polypharmacy.
- Compromised physical and cognitive abilities that reduce the capacity of an elderly person to maintain oral health.
- Lack of mobility to attend a dental surgery for regular preventive and restorative treatment.
- Severe salivary dysfunction can be a consequence of systemic diseases, anti-cholinergic medications, and head and neck radiotherapy. In the elderly and in particular in aged-care facilities, as already mentioned, polypharmacy is a common cause of salivary gland hypo-function due to the increased use of medicines to treat diseases associated with age and frailty.
- Increased intake of fermentable carbohydrates, aged-care facility staff and carers often rely on the increased use of snacks and sweet foods as a management tool to help control challenging behaviours and encourage the taking of medicines. Consequently, the frequency of eating may be many times greater than normal. As a general observation the relationship between decay, the frequency of eating and taking of medications with sweeteners is not understood by senior aged-care facility managers or the aged-care industry in general. It is an area where education is needed.
Levels of Dental Competence
Despite being co-operative, increasing mental and/or physical infirmity can result in the progressive loss of the ability of some patients to maintain their own oral care.
With these patients, inadequate oral hygiene, poor food clearance and the loss of saliva’s protective functions can result in major changes in risk factors, affecting disease initiation and progression.
An extremely difficult group to treat is the very frail who are no longer able to feed, dress or toilette themselves. They will usually reside in a high-care nursing section of an aged-care facility. Treatment offered at bedside by a visiting dentist is usually limited to emergency palliative care for their immediate problem.
No longer co-operative or competent; high-care dementia patients present particular problems. They are unable to maintain their own oral care and often show variation in behaviour from being fully compliant to non-co-operative. This behaviour may vary from day to day or even the time of day. Dementia patients will require regular ongoing interventions over their lifetime. Attempts to clean their mouth or carry out treatment can be very challenging. Oral care is best attempted by nursing staff with special training and skills in the oral care of dementia patients. There is high caries prevalence in aged-care facilities; a study was conducted of 243 residents in 19 aged-care facilities in Melbourne. (Chalmers JM, Carter KD, Spencer AJ. Caries incidence and increments in Adelaide nursing home residents. Special Care Dentist. 2005; 25(2):96-105.) The results showed that, with dentate residents: 67.9% had unrestored coronal caries with a mean 2.8 lesion and 77.4% had root caries with a mean 5.0 lesions.
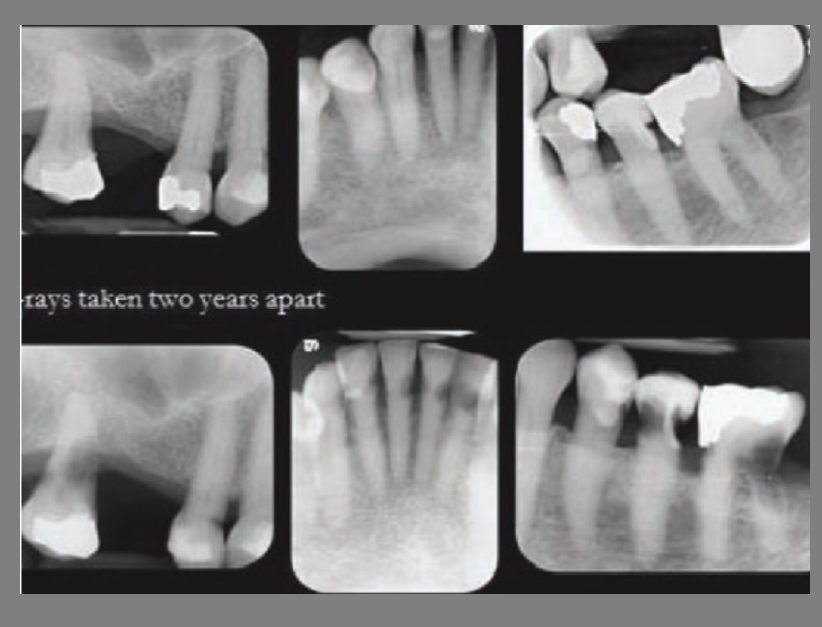
A combination of the above can lead to very rapid caries progression in the elderly; the examples below show rapid caries development over two years.