The use of Creighton Dental’s silver fluoride stannous fluoride combination (CSDS TM) to control and diagnose caries is well recognised. Teeth treated with CSDSTM can form a hard black matte on the treated surface known, as “The Black Diamond”. Creighton Dental has supercharged “The Back Diamond”, to the form “The Surface Silver Bullet’’. The application of silver fluoride followed by stannous fluoride currently produces a black matte, a visual signal caries is not progressing. Years of research and development has enhanced the silver fluoride, and stannous fluoride components in a novel and inventive way to produce a “Supercharged Black Diamond”. Ostensibly both black diamonds appear to be identical, but what lies on the surface of the “Supercharged Black Diamond “ of a treated carious surface lesion is a biochemical phenomenon, a world first method of synthesising nanao silver particles (AgNPs) on a carious lesion in situ , orally under physiological conditions of temperature, and pressure resulting in “The Black Diamond” transforming into, “The Surface Silver Bullet” .
The Silver Bullet helps mitigate the problem that sometimes occurs i.e., the depletion of silver ions one of the active bactericidal forces in CSDS. The diminished power of a CSDS treatment can be heralded by a visual colour change , from black matte to a lightening or reversion to the original caries lesion colour of yellow/brown, as described by Dr Graham Craig . (Craig et al., 2013) The chemical reduction of a silver fluoride dental solution, the preferred metal precursor, with an enhanced stannous fluoride, the preferred metal salt, or an organic reductant, reduces silver ions (Ag+) to silver atoms (Ag 0), that then produce nano silver particles (AgNPs). These can serve as a reservoir for silver ions, revitalising the deactivation process of the microorganisms present on carious lesion surfaces. The antibacterial properties of AgNPs are well recognised in the dental field. The tooth surface treatment method described, fulfils the need to maintain the uncompromised clinical efficacy of silver fluoride dental solutions, and shows the important role of the stannous ions in Creighton Dental’s CSDS’s stannous fluoride component.
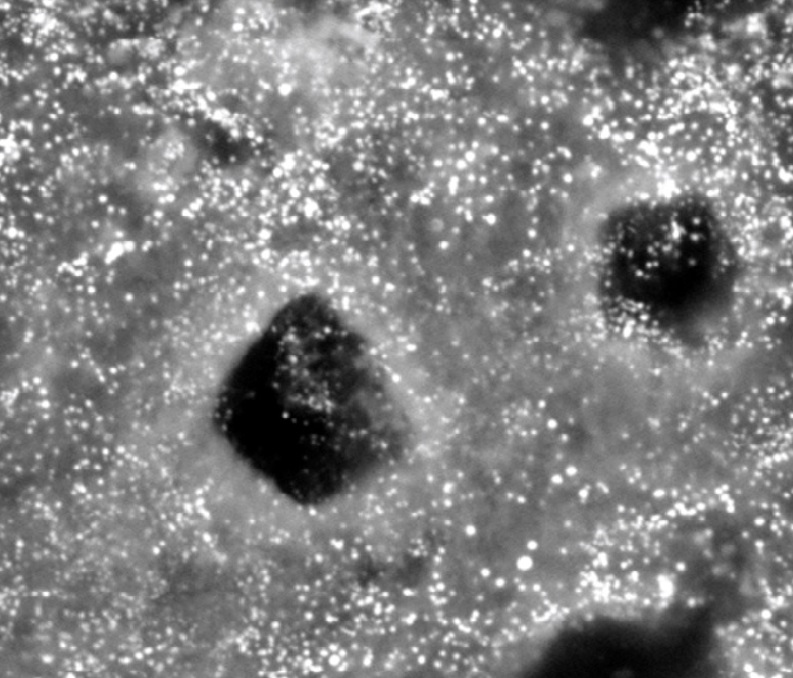
Fig 1 Scanning Electron Microscope (with a capability of nano size resolution) photograph of the “ Supercharged Black Diamond’ precipitate on a CSDS treated carious lesion, is inundated with white dots . The size of the white dots, and the fact they are silver, are consistent with nano silver .
Scanning Electron Microscope (SEM) sample images in Fig 1, are consistent with the white shining dots on the surface being nano silver particles (AgNPs).
Stannous fluoride has long been established as a topical fluoride with antimicrobial properties. The therapeutic efficacy of stannous fluoride depends on its stability. When free divalent (2+) stannous ions (Sn2+) in solution are oxidised to form tetravalent (4+) stannic ions (Sn4+), they no longer have protective properties. Stannous ions disassociate in water to form a white precipitate of tin (stannous) hydroxide, a process known as hydrolysis. All these chemical changes affect the bioavailability of stannous ions resulting in deactivation of an essential therapeutic ingredient.
Preparation of improved stannous fluoride (SnF2).
Creighton mitigates the inherent instability of the stannous ion, preparing stannous fluoride by dissolving 10%(w/v) stannous fluoride powder in between 1-100% (w/v) glycerol (glycerine), and between 1%-20% (w/v) sorbitol at a temperature of between 25-185 °C (degrees Celsius). This method produces a clear improved stabilised stannous fluoride dental solution with no white precipitate formation. This method produced an improved stable SnF2, which after age testing showed no observed change in stannous ion levels after aging at 55°C for 80 days, (the equivalent of 24 months of real time age testing in challenging humid and temperature environments), the stannous fluoride dental reductant solution was clear with no evidence of the characteristic white precipitate formed by oxidation of stannous ions.
This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1111/adj.12689
Summary
Background
Silver fluoride 40% followed by 10% stannous fluoride (AgF) has been used in dental practice in some parts of Australia for many years. This study compared the effectiveness of application of AgF with Atraumatic Restorative Technique (ART)* in managing cavitated carious primary molars
Methods
The study was a community effectiveness trial in two remote Aboriginal communities where AgF has been used for some time. Children between four and eight years of age with caries on primary molars were randomised by birth date to receive AgF or ART. There were 210 children who were included in the study with 384 eligible teeth. Children were followed up for periods between nine months and four years. Negative outcomes such as dental pain, extraction, use of antibiotics and more extensive restorative treatment were considered as the primary outcomes of the study
Discussion
This study found that use of the formulation 40% silver fluoride with 10% stannous fluoride was as effective as ART in treating dental caries among young children in a real life clinical setting in remote Australia. Both types of treatments resulted in very few complications. The null hypothesis (a hypothesis used in statistics that proposes that no statistical significance exists in a set of given observations) was supported.
The strength of this study included the use of a silver fluoride formula, one which has been more commonly used in Australia and does not have an ammonia smell. Treatment was undertaken in the posterior teeth of the primary dentition whereas most studies of silver diamine fluoride have treated anterior teeth. Other strengths were the comparison with an existing treatment (ART) and the evaluation of AgF in routine clinical practice. This meant that the results show success of the AgF rather than its value.
This study used a different formula than Silver diamine fluoride which gave results similar to SDF. The need for retreatment was regarded as a disadvantage in one result in this study but is recognised that it may be required as part of the treatment regime with AgF. Recent studies of silver diamine fluoride have suggested that biannual treatments are necessary to produce the best results with that agent. The use of the silver fluoride stannous fluoride combination enabled the maintenance of the primary dentition as well as ART.
This AgF treatment is simple and could be used by oral health therapists and hygienists. It was well accepted by children in this study. The black staining which results was not mentioned as a problem by the children in the study or their parents, and is clinically useful as an indicator of caries arrestment. Studies in vitro have raised the possibility that staining with SDF may be minimised with potassium iodide which could be investigated for AgF. AgF could also be used beneath glass ionomer cement fillings to reduce the appearance of staining or if the possibility of food packing was considered an issue.
In recent years the Hall Technique using preformed stainless steel crowns has been widely used to treat primary caries. This is also a treatment which does not require local anaesthetic and which reduces risk of major failure or pain compared to fillings. Research comparing use of silver fluoride with preformed stainless steel crowns would be useful. It would also be useful to conduct a cost-effective analysis regarding number of dental general anaesthetics prevented due to provision of AgF.
Results
Those negative outcomes were infrequent in both treatment groups. If retreatment with AgF is regarded as part of routine treatment, then the prevalence ratio of negative sequelae for children treated with AgF compared with those treated with ART was lower at 0.18
Conclusions Silver fluoride treatment for cavitated carious lesions in primary molars was as effective as the ART technique in this remote Indigenous population. It is an acceptable technique on very young and/or apprehensive patients and does not have the ammonium odour of SDF.
*The ART technique was developed as a treatment of dental caries, useful in areas where dental equipment and dentists were in short supply. The ART approach, is a relatively pain free, it includes both prevention and treatment of dental caries. ART procedure is based on excavating and removing soft diseased dentine using hand instruments only, and then restoring the tooth with an adhesive glass-ionomer material. (ART) has been endorsed by the World Health Organisation (WHO). ART requires fewer resources and is more acceptable than traditional dentistry in remote areas and for young children. However, even ART may be problematic and regarded as too intrusive for some Indigenous children. In addition, the materials required for ART require constant refrigeration which may not be feasible in some remote locations.
Comment It was wonderful to see Lauren Roberts article (Tues 12 March) “Fluoride alone no fix for NT teeth”. As a dentist who treated patients in the remote communities in North East Arnhem Land for more than 10 years, we and other clinicians were confronted by a massive backlog of untreated dental needs. The demand for immediate relief of pain was a priority, frequently requiring the extraction of untreatable teeth. However at the same appointment, we could easily apply the Silver Fluoride (now CSDS) whilst awaiting dental anaesthesia. This would result in a stable condition called “arrested caries”, which would enable the possible provision of restorative treatment in the future, when our clinical demands were hopefully reduced. This procedure was applied to both adult and children’s teeth, and being atraumatic, was very readily accepted by the patients. With the children especially, this was very empowering, as many of the teeth that required treatment were deciduous (baby) teeth that would be exfoliated with time. With the children in particular, this treatment saved many hospital visits where extensive travel costs and general anaesthetics would have been necessary to provide treatment. We called the treated teeth “Black Diamonds” and it was wonderful when walking through the community after work, to be greeted by the young patients, keen to show us their “black diamonds”! This same treatment is being used in aged care centres down south, where there is the need for dental treatment, but limited available treatment facilities. The treatment even has additional benefits in these situations as it makes keeping the gums healthy easier!
This
unflattering term alludes to the fact that a horse’s gums recede as it gets
older, and transfers this same phenomenon to humans. This transfer is not very
old, since until relatively recent times most adults who were old enough to
experience gingival recession had lost most of their teeth. It dates back to
the nineteenth century; the author William Thackeray used it in his novel The
History of Henry Esmond, Esq. (1852), “She was lean and yellow and long in the
tooth”.
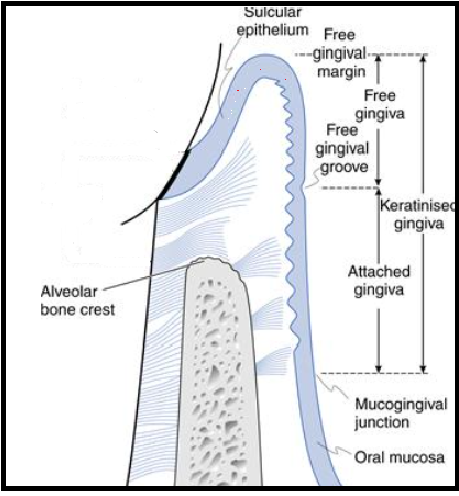
The attached gingiva
The attached gingiva is firm, resilient and tightly bound to the underlying alveolar bone and cementum by connective tissue fibres.
Gingival recession is common in a meaningful proportion of the adult population; it is present even in people with good oral hygiene. This suggests a complex array of causes (Joshipura et al. 1994) including anatomical and iatrogenic, as well as being closely associated with gingivitis and periodontal disease (Baker & Spedding 2002, Litonjua et al. 2005). The occurrence (gingival recession) increases in frequency with age; therefore, it is associated with age rather than a result of age. “Getting long in the tooth” is most likely due to loss of gingival attachment (Needleman 2015).
The significance is that all exposed root surfaces are at risk of root caries and this risk is greater in older dentate individuals. Regardless of the cause, gingival recession is increasing with age and root caries will increase as patients retain their teeth longer.
Geriatric patients residing in nursing homes are particularly vulnerable (Vigild 1989, Wyatt 2002, Simunkovic et al. 2005, Ferro et al. 2008) for a number of reasons including: polypharmacy, quantity and acid buffering ability of saliva, frequency of food intake, high use of food (especially fermentable carbohydrates) as a behavioural management tool, and lack of oral hygiene due to cognitive impairment.
Root caries anatomy
Root surfaces differ from enamel surfaces, due to root
surfaces (dentine) having a lower mineral content and a higher amount of
organic material (collagen). Because of
the smaller size of the apatite crystals, root surfaces are highly receptive to
mineral uptake in the oral environment (if there is good salivary flow with good
acid buffering capacity). This explains why exposed root surfaces usually
present a hyper-mineralised surface zone, the mineral content of which may be
higher than that of sound unexposed dentine (Selvig 1969). In vivo studies have
shown that topical treatments with fluoride may enhance mineral precipitation
in root surfaces (Furseth 1970).
Periodontal treatment including surgery , aggressive scaling and root planning may break or remove this hyper-mineralised area exposing the dentine tubules causing hyper-sensitivity and a roughened area that can accumulate biofilm/caries. Periodontal treatment may be counterproductive for the clinician who prefers to conserve the hyper-mineralised root surface (Heasman et al. 2017).
Caries management
From a clinical perspective the integrity of the root surface lesion should remain intact by adopting non-invasive treatment. All root surfaces are at risk of root caries, but areas that retain the biofilm are particularly vulnerable, these include: the cemento-enamel junction, mesial and distal interproximal surfaces and along the margins of restorations, especially at the gingival margin if the restoration is overhanging.
Treatments
Fluoride derivatives, Ammonia based 38% SDF was advocated as a treatment to arrest and prevent new dentine caries (Rosenblatt at al. 2009). This was attributed to the bactericidal properties of silver and fluoride’s ability to facilitate hyper-mineralisation (Nyvad et al. 1997); studies (Zhang et al. 2013, Li et al. 2016) found, annual SDF treatment may promote lesion arrest. Supporters of SDF treatment for root caries often ignore the potential harmful side effects, namely the mildly painful chemical burns on the oral mucosa that may last up to 48 hours (Rosenblatt et al.2009). To circumvent this side effect Deutsch (2016) used a different type of silver fluoride to treat root caries; he used a water-based 40% silver fluoride and 10% stannous fluoride. The advantage of this silver fluoride/stannous fluoride combination is it didn’t cause gingival burns. This was applied on a 3 to 4 month basis to multiple active root caries in frail elderly patients without causing any discomfort; furthermore, Deutsch suggested this approach to be suitable in the treatment of cognitively impaired elderly with behavioural problems where conventional treatment can be challenging if not impossible.
Conventional operative treatment of root caries should be
avoided, due to the relatively poor prognosis (Hu et al. 2005, Lo et al.2006,
Gil-Montoya et al. 2014) The majority of conventional restorations fail,
possibly due to patients having behavioural problems resulting in decreased
ability to cooperate; limiting the operator’s visibility, access, poor salivary
flow and acid buffering ability.
Recently high –viscosity glass ionomer cements (example product GC Equia
Forte TM) have become the
preferred choice due to the chemical bonding to root surfaces.
The need for effective root-surface treatments is illustrated by data from the UK. It has been reported that the percentage of dentate adults in all age groups in the UK and particularly those over 55 is increasing significantly over the decades (Steele et al. 2000, Fuller et al 2011). Future projections using 1988 and 1998 data predicted around 43% of adults over 85 in 2008 would retain at least one natural tooth. The actual figure turned out to be 53% (Fuller et al. 2011) far exceeding expectations. Furthermore, in the UK, adults over 55 that were retaining at least 21 natural teeth had increased by approximately 10% each decade from 30% in 1978 to 63% in 2009. Over the same period the mean number of teeth/individual had risen from 16 to 21.2 (Fuller et al. 2011); if this trend continues it is estimated by 2030 80% of adults in the UK will have at least 21 teeth with a mean of approximately 25 teeth. Given these predictions and the worldwide increase in the ageing population; root caries is set to become a very serious health issue for the world’s elderly citizens.
References
Baker, P. & Spedding, C. (2002) The aetiology of gingival recession. Dent Update 29, 59 –62. Deutsch, A. (2016) An alternate technique of care using silver fluoride followed by stannous fluoride in the management of root caries in aged care. Spec Care Dent 36, 85 –92.
Ferro, R., Besostri, A., Strohmenger, L.,
Mazzucchelli, L., Paoletti, G., Senna, A., Stellini, E. & Mazzoleni, S.
(2008) Oral health problems and needs in nursing home residents in Northern
Italy. Comm Health Dent 25, 231–236.
Frencken, J. E. (2014) The atraumatic restorative
treatment (ART) approach can improve oral health for the elderly; myth or
reality? Gerontology 31, 81 –82. (
Accessed June 2016)
Fuller, E.,
Steele, J., Watt, R. & Nuttall, N. (2011) Oral health and function – a
report from the Adult Dental Health Survey 2009. Available at:
http://www.hscic.gov.uk/catalogue/ PUB01086/adul-dent-heal-surv-summ-them-the
1-2009-rep3.pdf Accessed June 2016.
Furseth, R. (1970) A study of experimentally exposed
and fluoride treated dental cementum in pigs. Acta Odontol Scand 28, 833–850
Gil-Montoya, J. A., Mateos-Palacios, R., Bravo, M.,
Gonzalez-Moles, M. A. & Pulgar, R. (2014) Atraumatic restorative treatment
and Carisolv use for root caries in the elderly: 2year follow-up randomized
clinical trial. Clin Oral Investig 18,
1089-1095
Heasman PA, Ritchie M, Asuni A, Gavillet E, Simonsen
JL, Nyvad B. Gingival recession and root caries in the ageing population: a
critical evaluation of treatments. J Clinical Periodontol 2017; 44 (Suppl. 18):
S178–S193. doi: 10.1111/ jcpe.12676.
Hu, J. Y., Chen, X. C., Li, Y. Q., Smales, R. J. &
Yip, K. H. (2005) Radiation-induced root surface caries restored with
glass-ionomer cement placed in conventional and ART cavity preparations: results
after two years. Aust Dent J 50, 186–190.
Joshipura, K. J., Kent, R. L. & DePaola, P. F.
(1994) Gingival recession: intra-oral
distribution and associated factors. J Periodontol 65, 864–871.
Li, R., Lo, E. C. M., Liu, B. Y., Wong, M. C. M. &
Chu, C. H. (2016) Randomized clinical trial on arresting dental root caries
through silver diamine fluoride applications in community dwelling elders. J Dent
51, 15 –20.
Litonjua, L. A., Andreana, S. & Cohen, R. E.
(2005) Toothbrush abrasions and noncarious cervical lesions: evolving concepts.
CompendContin Educ Dent 26, 767–
768, 770-774, 776.
Lo, E. C. M., Loy, Y., Tan, H. P., Dyson, J. E. &
Corbet, E. F. (2006) ART and conventional root restorations in elders after 12
months. J Dent Res 85, 929–932.
Needleman, I. (2015)
Aging and the periodontium. In: Newman, M. G., Takei, H. H., Klokkevold,
P. R. & Carranza, F. A. (eds). Carranza’s Clinical Periodontology, 12th
edition, pp. 40–44, Philadelphia: Elsevier Saunders.
Nyvad, B., ten Cate, J. M. & Fejerskov, O. (1997)
Arrest of root surface caries in situ. J Dent Res 76, 1845–1853.
Rosenblatt, A., Stamford, T. C. & Niederman, R.
(2009) Silver diamine fluoride: a caries “silverfluoride bullet”. J Dent Res 88, 116–125.
Selvig, K. A. (1969) The formation of plaque and
calculus on recently exposed tooth surfaces. J Periodontol Res 4, S10–S11.
Simunkovic, S.
K., Boras, V. V., Panduric, J. & Zilic, I. A. (2005) Oral health among
institutionalised elderly in Zagreb, Croatia. Gerodontology 22, 238–241
Steele, J. G., Treasure, E., Pitts, N. B., Morris, J.
& Bradnock, G. (2000) Total tooth loss in the United Kingdom in 1998 and
implications for the future. Bri Dent J
189, 598–603..
Vigild, M. (1989) Dental caries and the need for
treatment among institutionalized elderly. Community Dent Oral Epidemiol 17, 102–105.
Wyatt, C. C. L. (2002) Elderly Canadians residing in long-term care hospitals: Part II. Dental caries status. J Can Dent Assoc 68, 359–363.
Zhang, W., McGrath, C., Lo, E. C. & Li, J. Y. (2013) Silver diamine fluoride and education to prevent and arrest root caries among community-dwelling elders. Caries Res 47, 284– 290.
The patients, an eighty-five year old medically compromised
male, with quadruple by- pass surgery (1990), and recently treated for a melanoma.
Currently on Warfarin (anticoagulant), Cardiprin (aspirin), Crestor (statin), Physiotems
(anti-hypertensive), Prazosin (alpha blocker, vasodilator) Micardis
(anti-hypertensive), Digoxin (for heart rhythm disorders)
As a result of polypharmacy (taking of 3 or more
pharmaceuticals), a liquid (saliva-like) is produced in the mouth, with
a pH as low as 5.0-5.8 (highly acidic); compared to moderately acidic saliva pH
6.0-6.6 and healthy saliva pH 6.8-7.8. The buffering action of saliva is
disrupted in these patients, the saliva produced, is a liquid with no buffering
ability, and is in fact, a source of
high acidity (pH 5.0-5.8), which usually can’t protect teeth surfaces
effectively; this level of acidity in the mouth favours demineralisation and/or
increasing colonisation by acidophilic bacteria. That is why we see rampant
caries in this patient and other elderly patients compromised by polypharmacy.
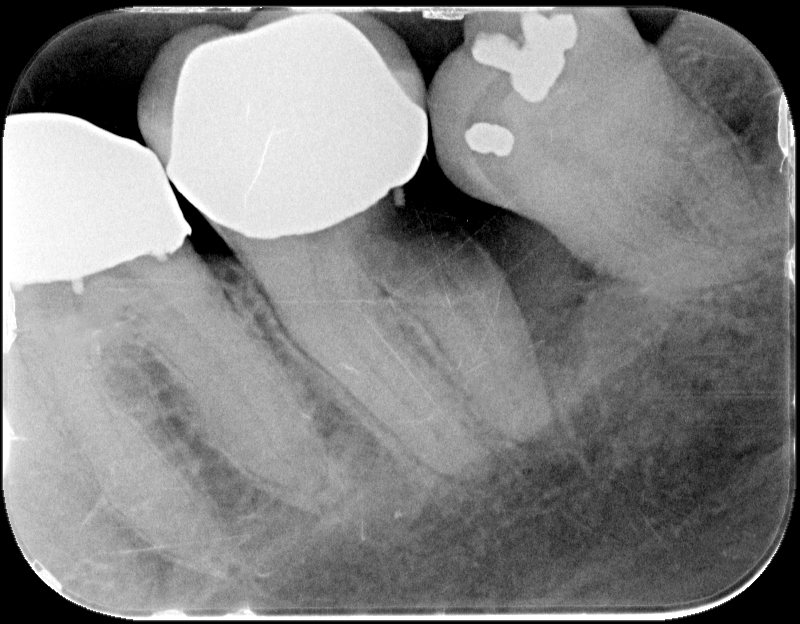
OPG 03/02/2015
Note a hint of caries on the distal of 37 and a large carious lesion on the mesial of tooth 17.
Bitewing radiograph (04/02/15) shows an area of translucency on the distal of 37, below the large restoration.
Periapical radiograph 14/06/2017 of 37, as a result of poor oral hygiene and dysfunctional saliva due to polypharmacy, shows very rapid caries progression from initial radiograph above date 04/02/2015
Tooth 37 17/10/2017; the patient was unable to maintain his oral hygiene and also because of the medical history it was decided to extract 37. With this in mind a consultation was held with the patient’s GP on how to best to manage the extraction given his dependence on anti-coagulants, and past difficulty in controlling bleeding after surgery. It was suggested that the patient be taken off Warfarin for at least 2 days before the surgery to manage the bleeding. His G.P agreed but insisted on maintaining some form of anticoagulant and prescribed Clexane to be taken on the day of the surgery. The tooth was extracted without complications, Spongestan placed in the wound and the socket sutured. The patient was not dismissed until the bleeding stopped and the wound was stable.
That night the wound began to bleed at around 7 pm continuing until 7am the next day (17/10/2017). He tried to arrest the bleeding by putting biting pressure on the wound with a gauze swab. The patient by his own accord discontinued the Clexane; after having bled all night and consulting with his GP in the morning, he was prescribed aspirin for that day and advised to recommence warfarin the next day which he did. Friday October 20, 2017; sutures were removed healing was progressing and Alvogyl placed in the socket.
Tooth 17 08/05/2018,was
grossly decayed and would, under normal conditions, have been extracted;
however, due to his history of abnormal bleeding even after packing the tooth
socket and suturing, and the insistence of his GP to continue anti-coagulants
before surgery, an alternative treatment was required. The crown was sectioned
just above the gingiva and the remaining root stumps treated with AgF and SnF2
(CSDS).
22/10/2018, on examination after seven months, the tooth was asymptomatic; there was a lightening of the black layer formed after initial treatment on the root stumps especially on the mesio-buccal root; indicating caries progression, AgF and SnF2 were re-applied. The patient will be re-examined in 4 to 6 months when the root stumps will be re-assessed.
Reproduced with the kind permission of Dr David Sheen AM BDS (Usyd MHP (UNSW) FICD and Dr. Robert Lilia BDent(Hons BEdu (USyd) Lyons Dental, Russell Lea, NSW.
A down-to-earth, field-tested presentation that will show how to benefit from the emerging silver fluoride wave with tips and traps on its implementation and use.
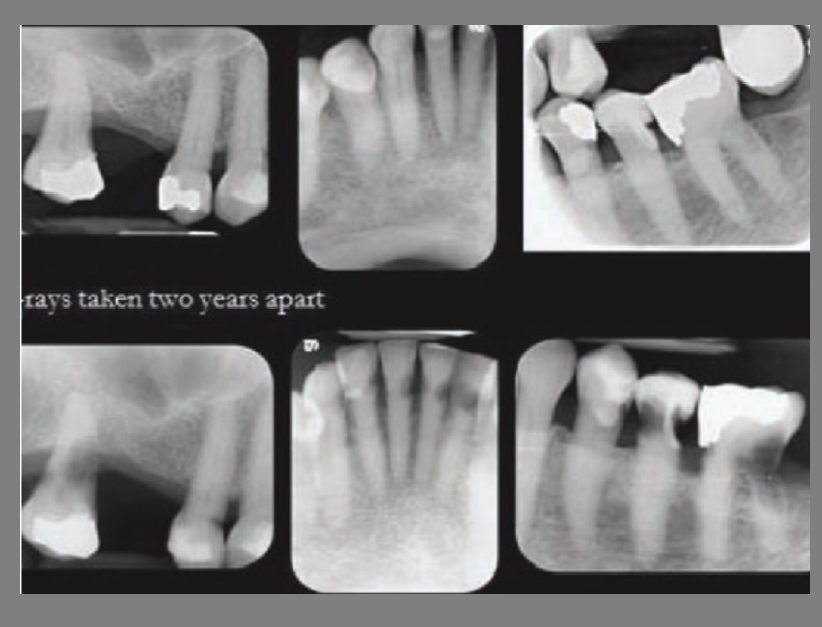
The rate of caries progression in aged care facilitiesis often rapid!
Conventional dental treatment in aged care facilities is often unsuccessful due to many compounding factors. Treatment of the very frail and elderly, especially those suffering dementia, is a relatively new field and often not handled well. Root surfaces are particularly vulnerable sites for dental caries in the frail and elderly. By middle age many root surfaces are exposed as a result of gingival recession, and each exposed surface is a potential site for future caries. The transition between a sound root surface and a grossly carious one can be extremely rapid, sometimes measured in months.
Factors contributing to raise the caries rates in aged-care facilities.
Often a catastrophic event such as a fall or a serious illness can impact and accelerate the deterioration of a person’s oral health.
As a result of polypharmacy, some patients produce liquid in their mouth, but instead of having the buffering effect of saliva, because of the changes in saliva flow and production; the pH of the resting saliva of these patients is as low as 5.0-5.8 which is highly acidic, compared to moderately acidic saliva pH 6.0-6.6 and healthy saliva pH 6.8-7.8.
The carbonate cycle that produces bicarbonate, responsible for the buffering action of saliva is disrupted in these patients, the saliva they produce is a liquid with no buffering ability, and is in fact a source of high acidity (pH 5.0-5.8), which usually can’t protect teeth surfaces effectively; this level of acidity in the mouth favours demineralization and/or increasing colonisation by acidophilic bacteria. That is why we see rampant caries in these elderly patients compromised by polypharmacy.
Compromised physical and cognitive abilities that reduce the capacity of an elderly person to maintain oral health.
Lack of mobility to attend a dental surgery for regular preventive and restorative treatment.
Severe salivary dysfunction can be a consequence of systemic diseases, anti-cholinergic medications, and head and neck radiotherapy. In the elderly and in particular in aged-care facilities, as already mentioned, polypharmacy is a common cause of salivary gland hypo-function due to the increased use of medicines to treat diseases associated with age and frailty.
Increased intake of fermentable carbohydrates, aged-care facility staff and carers often rely on the increased use of snacks and sweet foods as a management tool to help control challenging behaviours and encourage the taking of medicines. Consequently, the frequency of eating may be many times greater than normal. As a general observation the relationship between decay, the frequency of eating and taking of medications with sweeteners is not understood by senior aged-care facility managers or the aged-care industry in general. It is an area where education is needed.
Levels of Dental Competence
Despite being co-operative, increasing mental and/or physical infirmity can result in the progressive loss of the ability of some patients to maintain their own oral care.
With these patients, inadequate oral hygiene, poor food clearance and the loss of saliva’s protective functions can result in major changes in risk factors, affecting disease initiation and progression.
An extremely difficult group to treat is the very frail who are no longer able to feed, dress or toilette themselves. They will usually reside in a high-care nursing section of an aged-care facility. Treatment offered at bedside by a visiting dentist is usually limited to emergency palliative care for their immediate problem.
No longer co-operative or competent; high-care dementia patients present particular problems. They are unable to maintain their own oral care and often show variation in behaviour from being fully compliant to non-co-operative. This behaviour may vary from day to day or even the time of day. Dementia patients will require regular ongoing interventions over their lifetime. Attempts to clean their mouth or carry out treatment can be very challenging. Oral care is best attempted by nursing staff with special training and skills in the oral care of dementia patients. There is high caries prevalence in aged-care facilities; a study was conducted of 243 residents in 19 aged-care facilities in Melbourne. (Chalmers JM, Carter KD, Spencer AJ. Caries incidence and increments in Adelaide nursing home residents. Special Care Dentist. 2005; 25(2):96-105.) The results showed that, with dentate residents: 67.9% had unrestored coronal caries with a mean 2.8 lesion and 77.4% had root caries with a mean 5.0 lesions.
A combination of the above can lead to very rapid caries progression in the elderly; the examples below show rapid caries development over two years.
Alan A. Deutsch BDS, MPhil 1Bondi Junction, NSW, Australia Graham G. Craig MDS, PhD2 Camperdown, NSW, Australia
Correspondence Alan A. Deutsch, BDS, MPhil,
Bondi Junction, NSW2022, Australia.
Email: alan.deutsch@gmail.com
Abstract
An institutionalised high care dementia patient, who is unable to maintain his own oral health, presented with five lower anterior carious root stumps supporting a lower overlay denture. Due to limited co-operation, his root stumps were treated with only silver fluoride followed by stannous fluoride applied topically on a 4-monthly cycle. Almost one and a half years after his initial application, there were unexpected calculus formations on the root stumps accompanied by marked gingival inflammation and gingival hyperplasia. At this point prognosis was considered very poor. Because the patient’s cooperation was so poor, no attempt was made to remove the calculus deposits. Following continued topical applications directly to the area, there was evidence of a marked and unexpected improvement in gingival health. Some 4 years and 4 months after the initial application, the root stumps demonstrated a hard glossy surface surrounded by healthy gingival tissue. There had been no change in the patient’s oral care, minor changes to medications and there had been no operative or periodontal interventions.
KEYWORDS Aged care, arrest, dementia, minimally invasive, prevention, root caries, silver fluoride with stannous fluoride,